TL;DR:
- Clinical data provides essential human-subject evidence that supports the safety and efficacy of finished product formulations.
- Regulatory agencies require clinical studies on the final product, not just ingredient data, to validate marketing claims and ensure compliance.
Clinical data is defined as the direct, human-subject evidence that proves a finished product formulation is safe, effective, and performs as labeled. Without it, every claim on your product is an assertion without proof. Regulatory bodies including the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) demand that label claims be supported by competent, reliable scientific evidence derived from finished product studies, not ingredient lists alone. Understanding why clinical data supports formulation claims is not optional for researchers, formulators, or brand managers. It is the difference between a product that earns market trust and one that faces regulatory action.
Why clinical data supports formulation claims better than ingredient science
Ingredient-level science tells you what a compound can do in isolation. Clinical data tells you what your finished product actually does in a human body. That distinction is the entire argument.

A formulation is not a sum of its parts. Bioavailability, absorption rate, and tolerability all change depending on how ingredients are combined, processed, and delivered. A study on a single botanical extract does not transfer to a capsule, a softgel, or a topical cream containing that extract alongside emulsifiers, fillers, and preservatives. The finished formulation study is the only reliable method to confirm that the product in the consumer's hand performs as claimed.
This matters even more for dietary supplements. The FDA does not conduct pre-market review of supplement formulations. The burden of proof sits entirely with the brand. If a claim appears on the label, the company must hold evidence supporting it before the product ships. Clinical evidence from the finished product is the strongest form of that proof. It is what separates a defensible claim from a liability.
Brand managers often underestimate this gap. They commission ingredient studies, cite published research on isolated compounds, and assume that evidence transfers to their SKU. It does not. Regulators and plaintiffs' attorneys both know the difference.
How does clinical trial design substantiate formulation claims?
The design of a clinical trial determines whether the resulting data can actually support a specific claim. A poorly designed study produces data that is interesting but not actionable for regulatory or marketing purposes.
Crossover designs control for individual variability
Crossover studies compare a test formulation against a reference formulation within the same participants, eliminating the noise created by differences between individuals. Each participant receives both formulations in sequence, making the comparison direct and statistically cleaner. This design is the standard approach for bioequivalence and bioavailability studies because it isolates the formulation effect from everything else.
Fasting vs. fed conditions reveal real-world performance
Pharmacokinetic (PK) studies routinely test formulations under both fasting and fed conditions. The results can differ dramatically. A cannabidiol formulation study demonstrated that fed vs. fasted conditions produced measurable differences in absorption and peak plasma concentration. That finding directly affects what claims you can make about onset, duration, and bioavailability. If your label says "fast-acting," your clinical data must show it under the conditions consumers actually use the product.
Endpoints must match the claim
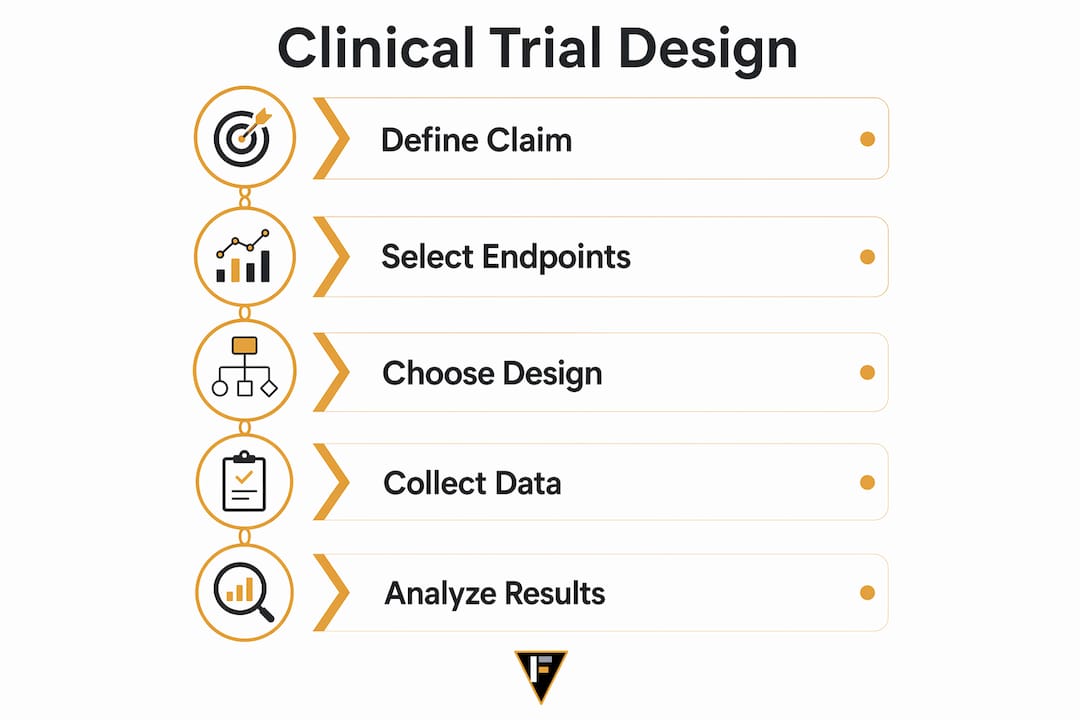
- Define the claim first. Write the exact label claim before designing the study. Every endpoint in the protocol should map directly to that claim.
- Select validated measurement tools. Use pharmacokinetic parameters like AUC (area under the curve) and Cmax for absorption claims. Use validated patient-reported outcome instruments for efficacy claims.
- Power the study correctly. Sample size must be large enough to detect a meaningful difference. Underpowered studies produce inconclusive data that regulators will reject.
- Pre-register the protocol. Registering on ClinicalTrials.gov before enrollment prevents post-hoc endpoint manipulation, which destroys credibility.
- Report negative findings. Selective reporting is a regulatory red flag and an ethical failure. Complete data packages build trust; cherry-picked summaries invite scrutiny.
Pro Tip: Design your clinical protocol with your regulatory submission in mind from day one. Retrofitting a study to meet FDA or EMA requirements after data collection is expensive and often impossible.
Why data quality and integrity are critical for claim validation
Collecting clinical data is not enough. The data must be accurate, complete, and traceable before it can support any claim.
Data integrity in pharmaceutical research encompasses accuracy, consistency, and reliability across the entire data lifecycle. High data integrity protects patient safety, supports correct therapeutic interpretation, and improves the probability of regulatory approval. A single data integrity failure can invalidate an entire study.
The components of trustworthy clinical data go beyond clean numbers:
- Accuracy: Every data point reflects what actually happened in the study, with no transcription errors or unauthorized alterations.
- Consistency: Data recorded at different time points and by different investigators follows the same definitions and measurement standards.
- Audit trails: Every change to a data record is logged with a timestamp and the identity of the person who made it. Regulators treat missing audit trails as evidence of potential manipulation.
- Metadata clarity: The context surrounding a data point, including collection method, instrument calibration, and site conditions, must be documented. Raw numbers without metadata are uninterpretable.
- Fitness for purpose: Data must be usable for the specific scientific and regulatory decisions it is meant to support.
"Effective clinical data management focuses on fitness for purpose, emphasizing the usability of data beyond mere cleanliness." — Quanticate Clinical Data Quality Research
Governance and metadata clarity are required beyond error-free data for the data to reliably support formulation claims. A dataset that is technically clean but lacks proper documentation of collection conditions cannot be used to substantiate a claim in a regulatory submission. This is where many brands fail. They generate data but cannot use it because the governance infrastructure was never built.
Clinical data vs. claims data: which actually validates formulations?
The terms "clinical data" and "claims data" are often confused, but they serve fundamentally different purposes in claim validation.
| Data Type | Source | Strength | Limitation | Best Use |
|---|---|---|---|---|
| Clinical data | Controlled trials, patient records | Direct safety and efficacy evidence | Expensive, time-intensive | Formulation claim substantiation |
| Claims data | Insurance, billing, pharmacy records | Broad population coverage | Lacks clinical detail | Healthcare utilization analysis |
| Real-world data | Electronic health records, registries | Large sample sizes | Observational, confounded | Post-market surveillance |
| AI-modeled data | Computational predictions | Fast, low cost | Requires clinical validation | Early formulation screening |
Claims data provides broad healthcare utilization information but lacks the clinical detail necessary to substantiate formulation safety and efficacy claims. It tells you how often a product category is prescribed or purchased. It does not tell you whether your specific formulation produced the effect stated on the label.
Real-world data from electronic health records adds population-level context but carries observational bias. It supplements clinical data after a product is on the market. It cannot replace controlled trial evidence during the approval or substantiation process.
AI-modeled data is the newest entrant. AI-designed formulations are now entering Phase I studies, with computational models predicting performance before human testing begins. This accelerates the path to clinical validation but does not eliminate the need for it. The model generates a hypothesis. The clinical trial confirms or refutes it.
What regulatory standards govern clinical evidence for formulation claims?
Regulatory requirements for clinical evidence differ by product category, but the direction of travel is consistent: more evidence, better documented, and more specific to the finished product.
For dietary supplements in the United States, the FDA requires that claims be supported by competent and reliable scientific evidence. The standard is not defined by statute with precision, but enforcement actions and Federal Trade Commission (FTC) guidance make clear that randomized controlled trials on the finished product carry the most weight. Ingredient studies and mechanistic data are supporting evidence, not primary substantiation.
For pharmaceutical and generic drug applications, the requirements are more specific:
- Bioequivalence studies must demonstrate that the test formulation delivers the same active ingredient at the same rate and extent as the reference product.
- Q3 microstructural comparisons are required for semi-solid dosage forms. Q3 evaluation criteria include viscoelasticity, particle size, and crystal morphology. These characteristics determine whether a generic cream or gel will perform identically to the reference product at the site of action.
- Pharmacokinetic studies under fasting and fed conditions are required when in vitro dissolution data alone cannot predict in vivo performance.
The EMA follows parallel logic through its bioequivalence guidelines, with additional emphasis on patient population subgroups and special dosage forms.
Pro Tip: Check the FDA's product-specific guidance documents before designing your bioequivalence study. These documents specify the exact study design, endpoints, and acceptance criteria for hundreds of individual drug products. Using them from the start prevents costly protocol amendments.
The trend toward AI integration in trial design is also reshaping regulatory expectations. Agencies are beginning to accept AI-assisted trial designs when the computational methods are transparent and validated. Brands that build standardized clinical data formats into their data infrastructure now will be positioned to take advantage of these pathways as they mature.
Key Takeaways
Clinical data is the only evidence type that directly validates formulation claims through controlled human-subject testing, and its quality, design, and regulatory alignment determine whether those claims will stand.
| Point | Details |
|---|---|
| Finished product studies are required | Ingredient science does not transfer to finished formulations; only finished product clinical data substantiates label claims. |
| Trial design determines claim validity | Crossover designs, matched endpoints, and pre-registered protocols produce data that regulators and courts will accept. |
| Data integrity is non-negotiable | Accuracy, audit trails, and metadata documentation are required for data to be usable in regulatory submissions. |
| Clinical data outperforms claims data | Claims and real-world data supplement but cannot replace controlled clinical trial evidence for safety and efficacy claims. |
| Regulatory standards are product-specific | FDA and EMA requirements vary by dosage form; Q3 microstructural criteria apply to semi-solids and must be addressed in study design. |
What I've learned about clinical data that most brands get wrong
Working across formulation projects, I've watched brands invest heavily in ingredient sourcing and then treat clinical validation as an afterthought. The logic seems sound: if the ingredients are proven, the product is proven. That reasoning fails every time it meets a regulator or a class action attorney.
The deeper problem is data readiness. More than half of AI projects in clinical development fail due to lack of data readiness. That statistic applies equally to brands trying to use their clinical data for regulatory submissions or marketing substantiation. The data exists, but it was never structured to be used. No common data model, no standardized ontology, no audit trail. The result is a dataset that cannot answer the question it was collected to answer.
My honest recommendation to brand managers: treat data governance as a product development cost, not an administrative burden. Build your data collection infrastructure before you start enrollment, not after you have results you cannot use. The benefits of data-driven formulations compound over time. Every study you run on a well-governed data platform produces evidence you can actually deploy.
The other pattern I see consistently is brands confusing statistical significance with regulatory sufficiency. A study can show a statistically significant effect and still fail to substantiate a specific label claim if the endpoint does not map to the claim language. Write the claim first. Design the study second. That sequence is not a formality. It is the entire logic of claim substantiation.
AI-assisted trial design is changing the speed of this process, but it is not changing the underlying requirement. Human-subject evidence from the finished product remains the standard. The tools are faster. The bar is the same.
— Ben
How Formlypro helps you build clinical data-backed formulations
Formlypro is built for researchers and brand managers who need more than a formulation database. The platform integrates compliance guidance, competitive analytics, and an 8-phase product development plan that takes you from ideation through production with regulatory requirements mapped at every stage.
When you reach the clinical validation phase, Formlypro's formulation analytics tools help you structure your data for regulatory submission and product compliance from the start. The AI Mockup designer handles packaging, and the competitor analysis module shows you exactly what clinical evidence competing products are using to support their claims. If you are ready to build formulations that can withstand regulatory scrutiny, start with Formlypro and see how the platform structures every phase of your product's clinical evidence strategy.
FAQ
Why can't ingredient studies alone support formulation claims?
Ingredient studies test isolated compounds, not finished products. Bioavailability, absorption, and tolerability all change in a complete formulation, so only finished product clinical data can substantiate label claims.
What is a crossover design in clinical trials?
A crossover design gives each participant both the test and reference formulation in sequence. This controls for individual variability and produces cleaner data for bioavailability comparisons between formulations.
What does Q3 evaluation mean for semi-solid formulations?
Q3 evaluation compares microstructural characteristics including viscoelasticity, particle size, and crystal morphology between a generic and reference semi-solid product. Regulatory agencies use these Q3 criteria as primary evidence for bioequivalence in creams and gels.
How does data integrity affect regulatory approval?
Data integrity failures including missing audit trails, inconsistent records, or undocumented metadata can invalidate an entire clinical study and block regulatory approval regardless of the underlying results.
Can AI replace clinical trials for formulation validation?
No. AI accelerates formulation screening and trial design, but Phase I clinical studies on human subjects remain required to confirm safety and efficacy. AI generates hypotheses; clinical trials confirm them.